
Chronic venous disease (CVD) and hemorrhoidal disease affect a large number of people. While these diseases manifest in different ways, they are caused by the same issue: inflammation of the veins.
CVD most often begins with discomfort in the legs, progressing gradually to varicose veins, edema, skin hyperpigmentation (discoloration), and ulcers in advanced stages. It is sometimes complicated by superficial or deep vein thrombosis (DVT), which is when a clot forms in a blood vessel and obstructs it. 22% of early-stage patients developed a venous leg ulcer within 6 years1.
CVD is strongly correlated with cardiovascular diseases and risk of all-cause mortality starting from the early stages of CVD and this risk increases with the progression of the disease2.
Moreover, CVD is similar with other disabling and impairing chronic diseases such as diabetes, obesity, and hypertension. With the progression of chronic diseases, the need for treatment increases while the quality-of-life decreases. Although these chronic conditions are typically considered as separate entities, they often co-exist which may be important in both understanding their pathophysiology and determining the best treatment strategy.
Venous diseases are the most common diseases in the world. According to a study published in 2021 in the Journal of Minerva Medica, Varicose veins are present in 25%-33% of female and 10%-40% of male adults3. The prevalence of CVD is highest up to 70% in Eastern Europe4. The disease consumes up to 2% of healthcare budgets in western countries5.
The main cause: poor circulation in the veins
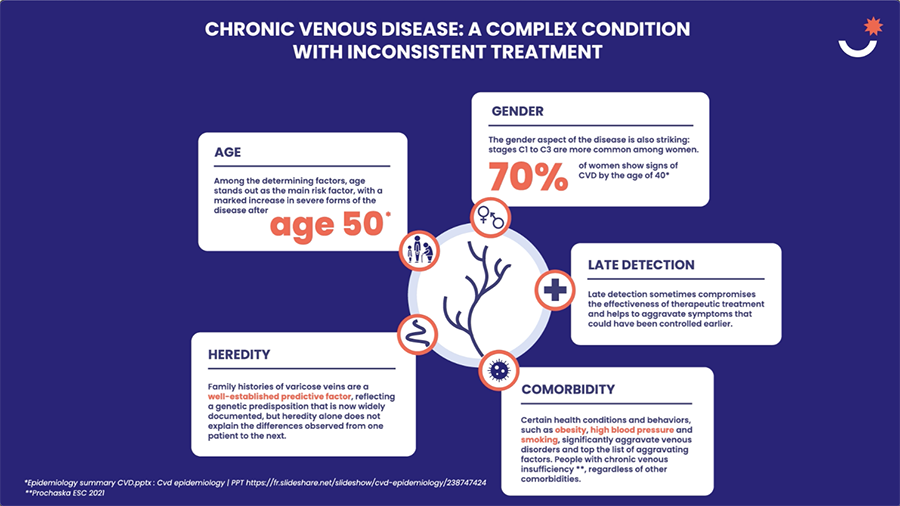
What are the risk factors for venous diseases?
Several risk factors can be associated with the onset of venous diseases. Patients can take action on those related to circumstances or lifestyle.
These include excess weight, level of physical activity, and standing for prolonged periods – all of which increase the likelihood of developing venous diseases. Furthermore, women are at greater risk than men, notably during pregnancy, the increased volume of the uterus compresses the veins in the abdomen, making it more difficult for venous blood to flow back up from the legs. Finally, venous disease can also be linked to genetic factors, and also increases the likelihood of developing this condition.
How are venous diseases treated?
Treatments are available today according to the stage of the disease. Patient education, physical activity, elevating the legs and keeping weight in check can slow its progression. Mechanical methods such as elastic compression stockings or socks can reduce the pressure of the blood on the valves. Use of venotonics can improve the symptoms associated with venous disease, as a complement to healthy lifestyle measures. Existing varicose veins are either surgically removed or sealed shut using radiofrequency or, laser, or the injection of a chemical solidifying agent (sclerotherapy)6.

About Servier
Servier works alongside health care professionals and patients to better understand venous insufficiency and treat the symptoms.
REMEMBER
[1] M R Cesarone, G Belcaro, A N Nicolaides, et al. ‘Real’ epidemiology of varicose veins and chronic venous diseases: the San Valentino Vascular Screening Project. Angiology. 2002;53(2):119-30. doi: 10.1177/000331970205300201.
[2] Prochaska JH, et al. Eur Heart J 2021; 42:4157-65 (https://pubmed.ncbi.nlm.nih.gov/34387673/)
[3] Management of chronic venous disorders of the lower limbs. Guidelines According to Scientific Evidence. Part I – International Angiology 2018 June;37(3):181-254 – Minerva Medica – Journals (https://www.minervamedica.it/en/journals/international-angiology/article.php?cod=R34Y2018N03A0181)
[4] Vuylsteke ME, et al. Angiology. 2018;69(9):779‒785 (https://pubmed.ncbi.nlm.nih.gov/29482348/)
[5] E Rabe, F Pannier. Societal costs of chronic venous disease in CEAP C4, C5, C6 disease. Phlebology. 2010:25 Suppl 1:64-7. doi: 10.1258/phleb.2010.010s09
[6] Insuffisance veineuse chronique, VIDAL, consulté le 10/03/2025 (https://www.vidal.fr/maladies/recommandations/insuffisance-veineuse-chronique-4045.html#prise-en-charge)